
Noticing more hair in the shower or on your brush? This guide clarifies postpartum hair loss versus female pattern hair loss (androgenetic alopecia)—what each looks like, when it starts, what to test, and the smartest next steps.
Wondering about postpartum hair loss? Pass this along to a friend who’s losing hair after birth.
Quick Take (The 30-Second Answer)
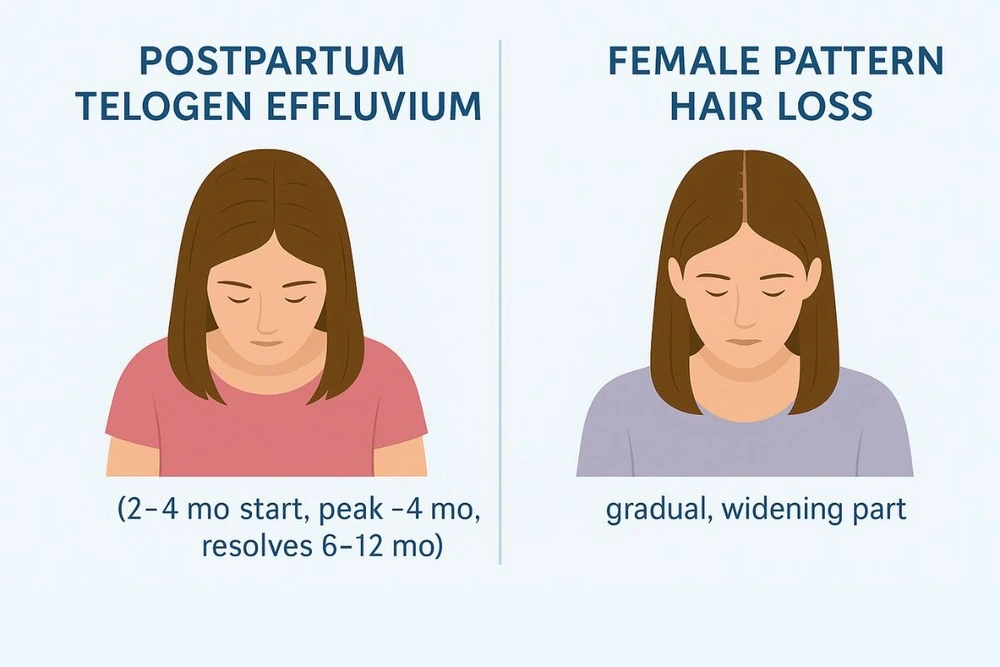
Postpartum hair loss = telogen effluvium (TE). It typically begins ~2–4 months after delivery, peaks around month 4, and resolves by 6–12 months for most people. If fullness isn’t back by 12 months, see a dermatologist.
Androgenetic alopecia (female pattern hair loss, FPHL) is gradual and progressive—classically a widening part/top thinning that doesn’t fully regrow without treatment.
Key divider: postpartum TE is diffuse shedding after a trigger (childbirth); FPHL shows patterned miniaturization and often persists. Accurate diagnosis = better results.
See also:Stress & Lifestyle Triggers • Hormonal & Health Causes • Genetics & Hair Loss
© hairimplants.net, 2025. All rights reserved. No unauthorised reproduction.
How To Tell Them Apart (at Home & With Your Doctor)
1) Pattern of loss
- Postpartum TE: Even, diffuse shedding from all over the scalp; your ponytail looks thinner suddenly. Baby hairs often sprout along the hairline during regrowth.
- FPHL: Widening part, density loss on the crown/central scalp; hairline often preserved. Progresses slowly without therapy.
2) Timing
- Postpartum TE: Starts 2–4 months after birth, peaks near month 4, then improves; most feel normal again by 6–12 months.
- FPHL: No obvious “trigger”; tends to creep in over years and may run in families.
3) What your clinician may check
- History & exam (including part-width photos/dermoscopy).
- Labs (case-by-case): TSH ± Free T4/T3 (thyroid), ferritin/iron studies if shedding is heavy or prolonged. These can mimic or magnify shedding postpartum.
Keep exploring causes here: Common causes of hair loss, Hormonal and health-related causes, Stress & lifestyle triggers
Why Postpartum Shedding Happens
During pregnancy, high estrogen keeps more hairs in anagen (growth). After delivery, hormones fall and many follicles shift together into telogen (resting)—then shed. It’s alarming, but it’s physiologic and temporary for most.
First-line Steps for Postpartum Hair Loss
- Be gentle: Looser styles, avoid tight ponytails/heat; wash/brush normally (you won’t “save” hair by skipping).
- Nutrition & iron: Eat protein-rich meals; if shedding is heavy or prolonged, ask about ferritin/iron testing.
- Cosmetic helpers: Volumizing cuts, strategic layers, tinted fibers while regrowth happens (usually visible by months 3–6 of recovery).
- When to seek care: If shedding is patchy, persists >12 months, or new symptoms arise (itch, scaling, bald patches), see dermatology to rule out androgenetic alopecia, alopecia areata, or scalp disease.
What About Minoxidil While Breastfeeding?
Evidence is limited. LactMed notes topical minoxidil likely poses low risk for healthy, full-term infants, but advises caution and to avoid with preterm/neonatal infants; many clinicians defer until after exclusive breastfeeding or use only if benefits clearly outweigh risks. Discuss personally with your obstetrician/dermatologist.
If it’s androgenetic alopecia (FPHL)
- What to expect: Slowly progressive thinning (part/crown). Genetics play a major role.
- Evidence-based options:
- Topical minoxidil (2% or 5%) is first-line for women (timing around breastfeeding as above).
- Low-level laser therapy and PRP as adjuncts in selected cases.
- Oral therapies (e.g., spironolactone, finasteride off-label in women after childbearing; specialist supervision required).
- Hair transplantation for stable, well-selected cases with adequate donor supply.
Learn more: How genetics influence hair loss
Postpartum TE + Underlying FPHL Can Coexist
Some people notice intense shedding after childbirth and an underlying pattern loss becomes obvious. Your clinician may treat TE supportively while starting long-term FPHL strategies once it’s safe and appropriate.
See Top-Rated Clinics
Prefer a diagnosis-first approach? Browse neutral, vetted clinics that manage genetic hair loss with medical therapy (and surgery if needed). Filter by credentials, outcomes, and follow-up care. → See top-rated clinics
Hair Enhancement Resources & Guides
- Common causes of hair loss
- Stress & Lifestyle Triggers for Hair Loss
- Hormonal & Health-Related Causes of Hair Loss
- How Genetics Influence Hair Loss
- Thyroid and Hair Loss: Symptoms & What to Test
FAQ: Postpartum Hair Loss
Bottom Line
Post-baby shedding is common—and usually temporary. If hair loss starts 2–4 months after delivery and eases by 6–12 months, you’re likely dealing with postpartum telogen effluvium. Persistent widening at the part/top points to androgenetic alopecia, which benefits from diagnosis and treatment planning. Work with a dermatologist, consider targeted labs, and re-evaluate at the one-year mark. With the right plan, postpartum hair loss doesn’t have to be confusing—treat the cause, support regrowth, and track progress with monthly photos.
Was this useful? Share this postpartum hair loss guide with a new mom.
References
- American Academy of Dermatology. Hair loss: Diagnosis and treatment.
- American Academy of Dermatology. Female pattern hair loss (FPHL): overview & signs.
- Johns Hopkins Medicine. Postpartum Hair Loss: When it starts and why.
- Cleveland Clinic. Postpartum Hair Loss: Causes, treatment & what to expect.
- StatPearls (NCBI). Telogen Effluvium—definition, triggers, evaluation. Updated 2024.
- LactMed (NCBI Bookshelf). Minoxidil—use during lactation (topical).Updated 2024.
- Harvard Health Publishing. Treating female pattern hair loss (patterns, options). Updated 2024.
- Harvard Health Publishing. Thinning hair in women: why it happens and what helps. Updated 2024.
- Malkud S. Telogen Effluvium: A Review. Indian J Dermatol Venereol Leprol (PMC). Timing (2–3 months post-trigger) and natural history.
- Cheng T, et al. Diagnostic value of serum ferritin for telogen effluvium. J Cosmet Dermatol (PMC).
Medical Disclaimer: The content on hairimplants.net is for informational purposes only and should not be considered medical advice. It does not replace a professional medical consultation, diagnosis, or treatment. Readers are encouraged to seek guidance from a qualified healthcare provider before making any decisions about hair restoration treatments. Hairimplants.net accepts no liability for actions taken based on the information provided.
Affiliate Disclosure: Hairimplants.net may contain affiliate links. If you click a link and make a purchase, we may earn a small commission at no additional cost to you. This helps us keep our content free and research-based. Our editorial opinions are independent and not influenced by partnerships. We do not accept payment for favorable reviews or rankings. Links to medical sources are non-affiliate.





