
Seeing your part line widen—or shedding everywhere at once? This guide clarifies female pattern hair loss vs diffuse thinning so you can spot the difference quickly, order the right tests, and choose treatments that actually help.
Female pattern hair loss vs diffuse thinning — spot the difference fast, see what to test, and choose the right next steps.
Quick answer (30 Seconds)
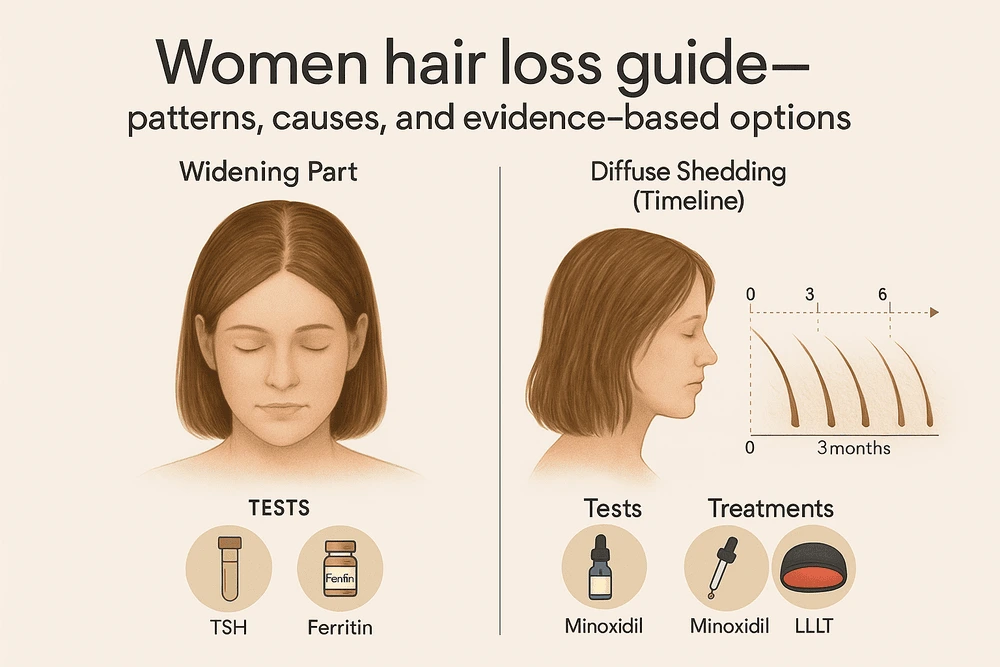
Female Pattern Hair Loss (FPHL): Gradual, patterned thinning—widening part and crown density loss; hairline usually preserved. Driven by follicle miniaturization.
Diffuse Thinning / Telogen Effluvium (TE): Sudden, uniform shedding from all over the scalp, often 2–3 months after a trigger (illness, postpartum, surgery, crash diet, new meds). Usually self-limited after the trigger resolves.
First-line labs (case-by-case): TSH ± Free T4/T3 (thyroid), ferritin/iron studies if shedding is heavy or prolonged.
They can coexist: Postpartum or illness-related TE may unmask underlying FPHL—use photos and timelines to tell them apart.
New here? Read our deep dives: Common causes of hair loss · Hormonal & health causes · Hair loss prevention routine
© hairimplants.net, 2025. All rights reserved. No unauthorised reproduction.
How to tell FPHL from diffuse thinning (what you see in the mirror)
Female Pattern Hair Loss (FPHL)
- Look: A widening central part that extends back; the top/crown looks see-through in photos. The frontal hairline is often preserved.
- Feel: Slow and steady over months/years; ponytail gradually shrinks.
- Clues: Family history of pattern loss; scalp generally looks normal (no scarring or inflammation).
- Dermatoscopy: Shows hair miniaturization (more thin hairs among thicker ones).
Diffuse Thinning / Telogen Effluvium (TE)
- Look: Hair comes out from everywhere—brush, pillow, shower drain; the part may look a bit wider simply because overall volume drops.
- Timing: Begins ~2–3 months after a trigger: fever/illness, childbirth, surgery, rapid weight loss, major stress, or new medications.
- Course: Often self-resolves once the trigger is addressed; density returns slowly as the cycle resets.
Related reads: Stress & lifestyle triggers · How genetics influence hair loss
A Practical At-Home Checklist
- Photograph your part and crown monthly in the same lighting.
- Timeline the last 6 months: illness, high stress, diet changes, childbirth, new meds.
- Ponytail test: sudden drop in circumference → think TE; slow decline → think FPHL.
- Edges check: receding frontal hairline is less typical in FPHL; if present, get a dermatology review.
What to Test (Targeted, Not a Shopping List)
- Thyroid: TSH ± Free T4/T3 when symptoms (fatigue, cold/heat intolerance, cycle changes) or heavy diffuse shedding suggest a thyroid link.
- Iron: Ferritin + iron studies + CBC—low ferritin can amplify TE even without frank anemia.
- Consider vitamin D, B12, zinc only if history/diet/exam point that way.
- Medication review: anticoagulants, retinoids, some antidepressants/anticonvulsants, antithyroid drugs and others can trigger TE—review all changes in the last 6 months.
Treatment Pathways (Match Therapy to The Cause)
If it’s mostly FPHL (pattern loss)
- Topical minoxidil is first-line.
- Women’s 5% foam once daily or 2% solution twice daily (label regimens).
- Expect an early shed in weeks 2–8; visible gains often need 3–6+ months.
- Women’s 5% foam once daily or 2% solution twice daily (label regimens).
- Expect an early shed in weeks 2–8; visible gains often need 3–6+ months.
- Prescription options (dermatologist-guided):
- Spironolactone (common antiandrogen for women).
- Finasteride/dutasteride in selected post-menopausal women (off-label; specialist care).
- Adjuncts: Low-level laser therapy (LLLT) 3–4×/week; PRP in selected cases; microneedling (timed away from topicals).
- Surgical option: Hair transplantation for stable cases with adequate donor hair—after medical therapy optimizes surrounding density.
If it’s mostly diffuse thinning (TE)
- Fix the trigger: recover from illness, correct thyroid/iron, stop crash diets, discuss medication alternatives with your prescriber.
- Be patient with the timeline: shedding eases first; density follows over months.
- Supportive care: gentle hair routine, treat dandruff/inflammation, consider cosmetic fibers while regrowing.
Day-to-day help: Everyday hair care routine · Daily scalp care routine · Non-surgical methods
When Both Happen at Once
It’s common to have a TE episode (e.g., postpartum) over an underlying FPHL. You might notice dramatic shedding, then the part still seems wider months later. In these cases, clinicians support recovery from TE and start long-term FPHL therapy to protect density.
Realistic Expectations & Tracking
- 4–8 weeks: TE begins to calm; minoxidil may cause temporary early shed.
- 3–6 months: First visible thickening for responders (minoxidil/LLLT/antiandrogens).
- 6–12 months: Best checkpoint to judge your plan—tune with your dermatologist.
- Photos win: same angle, distance, and lighting beat memory every time.
See Top-Rated Clinics
Prefer a diagnosis-first approach? Browse neutral, vetted clinics that manage genetic hair loss with medical therapy (and surgery if needed). Filter by credentials, outcomes, and follow-up care. → See top-rated clinics
Hair Enhancement Resources & Guides
- Common causes of hair loss
- Hormonal and health-related causes
- Hair loss prevention routine
- Everyday hair care routine
- Daily scalp care routine
- How genetics ingluence hair loss
FAQ
Bottom Line
You don’t need to guess between female pattern hair loss vs diffuse thinning. Map your pattern, check recent triggers, run targeted labs (thyroid/iron when indicated), and match treatments to the cause. With a simple, consistent plan—and help from a dermatologist when needed—you can protect density and see progress over time. See top-rated clinics here.
Was this helpful? Share this female pattern hair loss vs diffuse thinning guide with someone who’s unsure what’s causing their shed.
References
- American Academy of Dermatology (AAD). Hair loss: Diagnosis & treatment.
- AAD. Female pattern hair loss (FPHL): signs & treatment.
- StatPearls (NCBI). Telogen Effluvium.
- StatPearls (NCBI). Androgenetic Alopecia.
- Harvard Health Publishing. Thinning hair in women: why it happens and what helps.
- DermNet NZ. Diffuse alopecia.
Medical Disclaimer: The content on hairimplants.net is for informational purposes only and should not be considered medical advice. It does not replace a professional medical consultation, diagnosis, or treatment. Readers are encouraged to seek guidance from a qualified healthcare provider before making any decisions about hair restoration treatments. Hairimplants.net accepts no liability for actions taken based on the information provided.
Affiliate Disclosure: Hairimplants.net may contain affiliate links. If you click a link and make a purchase, we may earn a small commission at no additional cost to you. This helps us keep our content free and research-based. Our editorial opinions are independent and not influenced by partnerships. We do not accept payment for favorable reviews or rankings. Links to medical sources are non-affiliate.





