
Trying to decide between the two most-used oral 5-alpha-reductase inhibitors? This comparison of finasteride vs dutasteride explains how they work, which one grows more hair, common side effects, and smart safety checks—so you can talk to your clinician with confidence.
Finasteride vs dutasteride — an evidence-based breakdown of efficacy, side effects, and how to choose.
The Headline
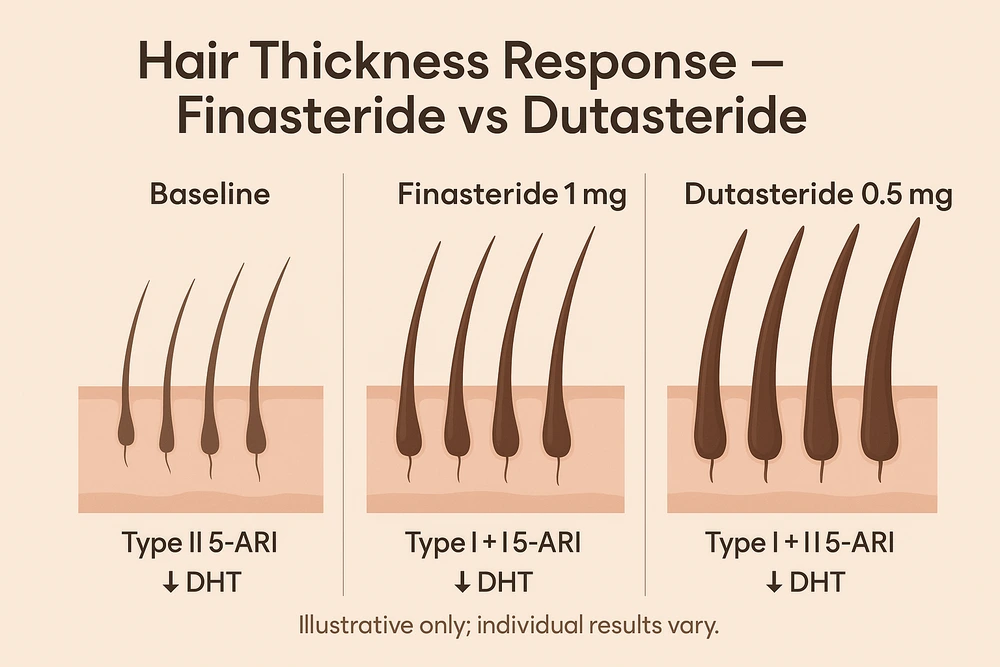
Both reduce DHT, the hormone that miniaturizes follicles in pattern hair loss. Finasteride blocks type II 5-alpha-reductase; dutasteride blocks type I + II, leading to deeper DHT suppression overall.
Effectiveness: Multiple trials and meta-analyses suggest dutasteride improves hair counts and global assessments more than finasteride, with broadly similar overall adverse-event rates in studies.
Approvals: For hair loss, finasteride 1 mg is FDA-approved (men). Dutasteride is FDA-approved for BPH; its use in male AGA is off-label in many countries (approved for AGA in some regions like South Korea/Japan). Always follow local regulations.
See also:Everyday hair care routine · Daily scalp care routine · Non-surgical methods
© hairimplants.net, 2025. All rights reserved. No unauthorised reproduction.
How They Work (and Why That Matters)
- Finasteride 1 mg daily selectively inhibits type II 5-alpha-reductase (high in hair follicles and prostate). Result: lower scalp/serum DHT, slowing miniaturization.
- Dutasteride 0.5 mg daily inhibits type I + II enzymes and has a very long half-life (~5 weeks), keeping DHT down more persistently (~90–95% serum DHT reduction reported in pharmacology studies).
Which grows more hair?
The clinical data (high level)
- Head-to-head RCT (24 weeks, n≈400): Dutasteride 0.5 mg outperformed finasteride 1 mg and placebo in hair counts and investigator assessments; finasteride beat placebo.
- Meta-analysis (2019, 7 studies): Dutasteride > finasteride for efficacy; adverse-event rates similar between groups.
- Long-term/real-world data: Observational cohorts suggest better improvement on dutasteride with similar or lower sexual AE rates vs finasteride, but these are not RCTs.
Bottom line: If you tolerate it and your clinician agrees, dutasteride is often the more potent choice for male pattern hair loss. Finasteride still works well for many and is on-label in more markets.
Dosing at a Glance (Typical Dermatology Practice)
- Finasteride (men): 1 mg orally once daily. Label-approved for male AGA. Expect evaluation at 3–6 months.
- Dutasteride (men, off-label for AGA): 0.5 mg orally once daily is common. Some clinics test intermittent regimens (e.g., 2–3×/week) to balance efficacy and AEs; early randomized pilots exist but evidence is still maturing.
- Women: Oral 5-ARIs are not routinely used pre-menopause; selected post-menopausal women may be treated off-label under specialist care with informed consent and contraception where applicable. See your dermatologist.
Layering treatments helps. Consider topical minoxidil, LLLT, microneedling (timed properly), and address thyroid/iron if deficient. See: Hair Loss Prevention Routine · Microneedling: How Often & Needle Size · Non-surgical methods
Side Effects & Safety: Where They Overlap, Where They Differ
Common across both (usually mild/transient):
- ↓ libido, erectile/ejaculatory symptoms; breast tenderness or enlargement; mood changes in some; rash. Discuss promptly with your clinician. (Rates vary across studies.)
Regulatory safety notes you should know:
- PSA reduction: Both drugs lower PSA, complicating prostate-cancer screening; clinicians often double the measured PSA to estimate baseline while on therapy. Don’t self-interpret—talk to your doctor.
- High-grade prostate cancer warning: Both labels include warnings based on historical trials in BPH populations. Clinicians individualize risk/benefit.
- Pregnancy handling: Tablets/capsules are contraindicated in pregnancy and should not be handled by pregnant people if crushed or leaking.
- Mood/suicidality: In 2025, the European Medicines Agency confirmed suicidal thoughts as a recognized adverse effect for finasteride 1 mg, adding risk communication tools; precautionary language was also added to dutasteride labeling. If mood changes occur, stop and seek care.
Half-life & washout: Dutasteride’s ~5-week half-life means slower washout and longer persistence of effects/side effects than finasteride (hours to a day). Plan changes with your clinician.
Practical Chooser: Finasteride vs Dutasteride
Choose finasteride if you want:
- On-label therapy for male AGA in many regions; shorter half-life (easier to stop/adjust).
Choose dutasteride if you need:
- More potent DHT suppression and, in studies, greater hair gains—accepting off-label use for AGA in some countries and a longer half-life.
For many, the path is start with finasteride, monitor photos and side effects, and escalate to dutasteride if results plateau and you and your clinician agree on the trade-offs.
What to Expect (Timeline)
- 3 months: shedding stabilizes; early signs on photos.
- 6–12 months: visible thickening if you’re a responder.
- Keep going: benefits persist with continued use; stopping leads to gradual loss of gains over months.
Monitoring Checklist (Bring to Your Visit)
- Baseline photos (front/top/crown) in consistent light.
- Medical history (sexual function, mood, fertility plans, prostate history).
- Discuss PSA strategy if age/risk makes sense.
- Adjunct plan (minoxidil/LLLT/microneedling; treat dandruff; correct iron/thyroid if needed).
See Top-Rated Clinics
Prefer a diagnosis-first approach? Browse neutral, vetted clinics that manage genetic hair loss with medical therapy (and surgery if needed). Filter by credentials, outcomes, and follow-up care. → See top-rated clinics
Hair Enhancement Resources & Guides
- Everyday hair care routine
- Daily scalp care routine
- Non-surgical methods
- Hair loss prevention routine
- Microneedling for Hair: How Often & Needle Size
FAQ: Finasteride vs Dutasteride
Bottom Line
For androgenetic alopecia, both drugs help—finasteride is widely approved and a strong first step; dutasteride is more potent and often more effective but is off-label for AGA in many places and has a longer half-life. Decide with your dermatologist, monitor photos and side effects, and combine with topical/adjunct options for best results.
Was this helpful? Share this finasteride vs dutasteride guide with someone comparing options.
References
- Harcha WG, et al. Randomized, active- and placebo-controlled study comparing dutasteride 0.5 mg vs finasteride 1 mg in AGA (24 weeks).
- Zhou Z, et al. Meta-analysis: Dutasteride appears more effective than finasteride with similar AE rates. J Dermatolog Treat. 2019.
- Amory JK, et al. Pharmacology: Dutasteride inhibits type I + II; ≈95% serum DHT reduction. J Clin Endocrinol Metab. 2008.
- PROPECIA (finasteride 1 mg) label: PSA lowering and safety information. FDA.
- AVODART (dutasteride) label: dual enzyme inhibition; half-life ~5 weeks; warnings. FDA.
- Choi GS, et al. Long-term observational cohort: greater effectiveness of dutasteride vs finasteride; AE occurrence similar or lower. 2022.
- EMA safety communication (2025): Suicidal thoughts recognized as side effect of finasteride 1 mg; label and patient card updates; cautionary language for dutasteride.
- AAD. Hair loss: Diagnosis & treatment — role of 5-ARIs in AGA care.
Medical Disclaimer: The content on hairimplants.net is for informational purposes only and should not be considered medical advice. It does not replace a professional medical consultation, diagnosis, or treatment. Readers are encouraged to seek guidance from a qualified healthcare provider before making any decisions about hair restoration treatments. Hairimplants.net accepts no liability for actions taken based on the information provided.
Affiliate Disclosure: Hairimplants.net may contain affiliate links. If you click a link and make a purchase, we may earn a small commission at no additional cost to you. This helps us keep our content free and research-based. Our editorial opinions are independent and not influenced by partnerships. We do not accept payment for favorable reviews or rankings. Links to medical sources are non-affiliate.





